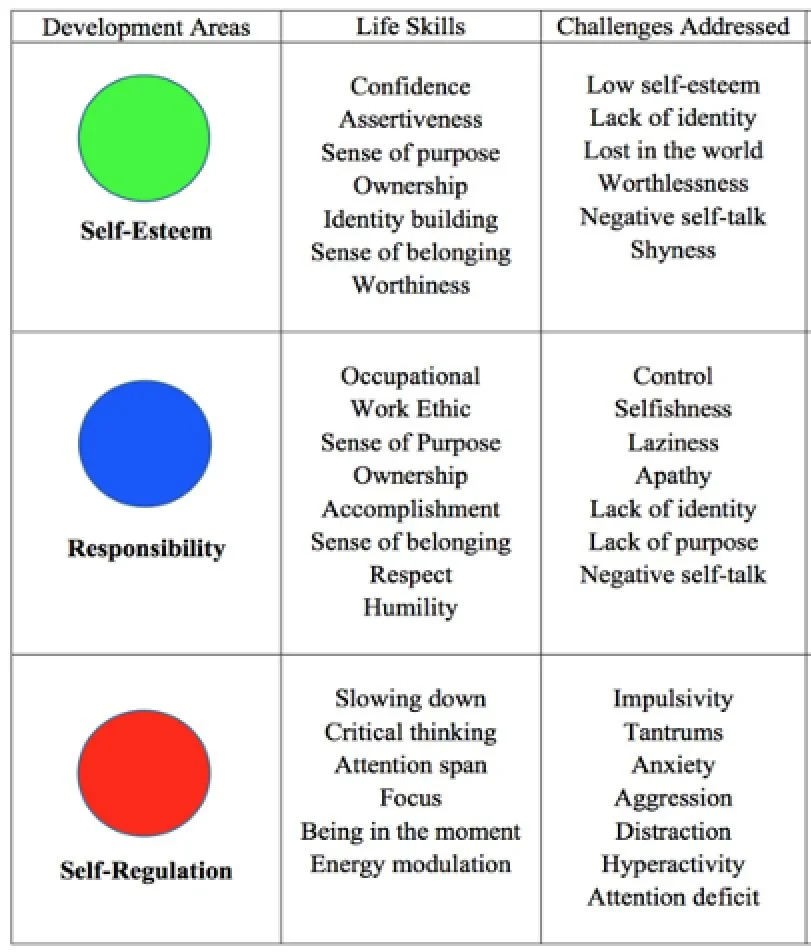
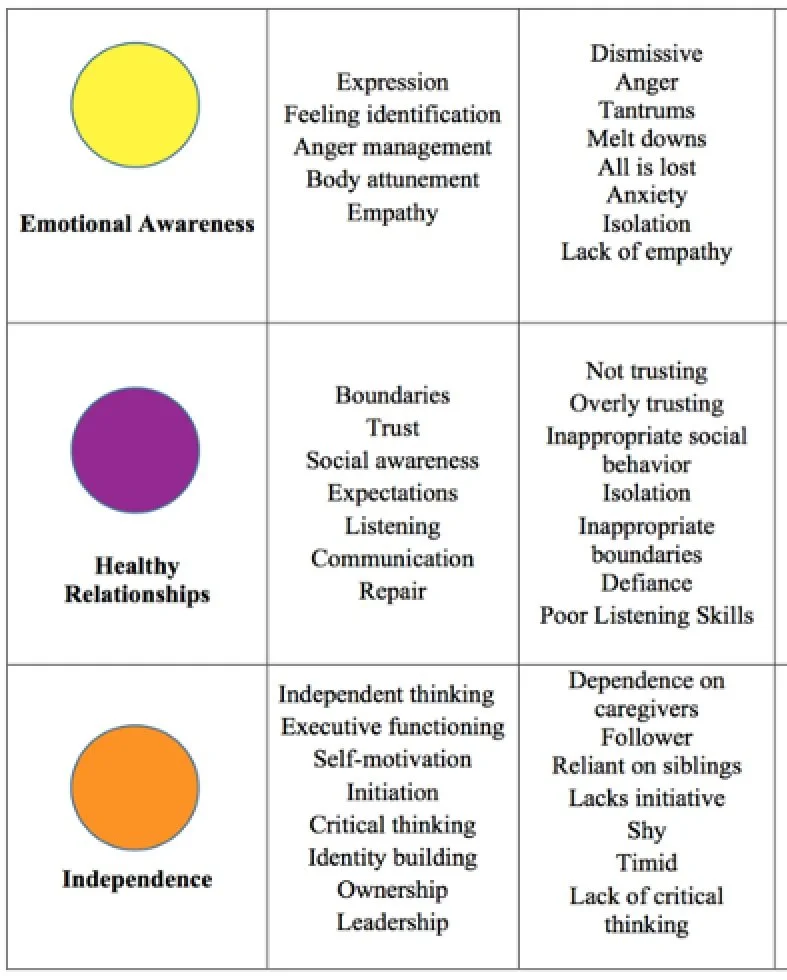
Stable Moments Activity Log Mentor First & Last Name * First Name Last Name Child First Name * First Name Last Name Date * MM DD YYYY What was the plan or selected activities for today? * How did it go? How did your activities work towards the life skills shown on the left? * Any questions, guidance needed, or issues you need support with? In thinking about the 60 minutes you spent with your kiddo. What percent would you say they experienced peace? * 0% 25% 50% %75 100% In thinking about the 60 minutes you spent with your kiddo. What percent would you say they experienced joy? * 0% 25% 50% 75% 100% Did your participant experience a moment(s) of peace and/or joy during your session? * Yes No Describe the moment(s) of peace and/or joy. Thank you!